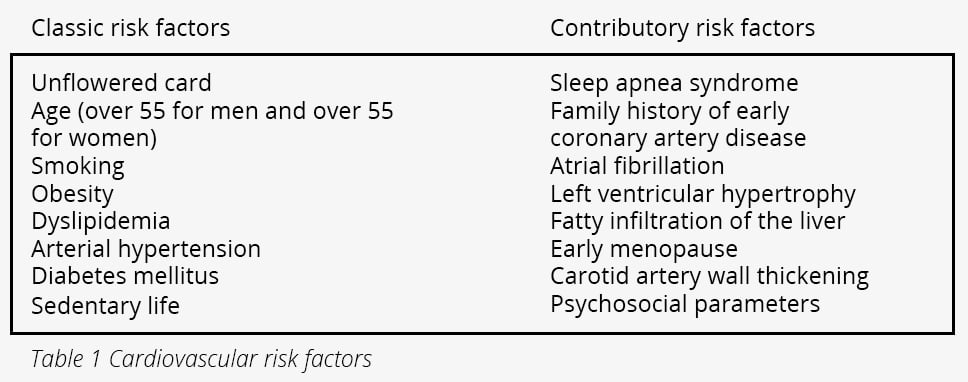

Cholesterol is a structural component of cell membranes and a raw material for the production of steroids and other hormones by the body. Of the measured cholesterol, 50% comes from the diet and the remaining 50% is produced by the body. Increased intake of saturated fatty acids from animal fats, red meat, fatty cheeses and obesity are common causes of dyslipidemia. In addition, genetically predisposed individuals have dyslipidemia despite not having the above characteristics. Dyslipidemia is a major cardiovascular risk factor, particularly in people aged between 30 and 60 years. Coronary heart disease is the leading cause of death in our country, with neoplasms a distant second.
Normal lipid levels are largely determined by LDL cholesterol levels and cardiovascular risk stratification. Low risk individuals have a target LDL <115 mg/dl , moderate risk individuals have a target LDL <100 mg/dl, high risk individuals have a target LDL <70 mg/dl and very high risk individuals such as those who have had a myocardial infarction or a stroke have a target LDL <55 mg/dl.
In addition to the parameters mentioned above, lipoprotein A Lp(a) is an independent cardiovascular risk factor. It is recommended to be measured at least once during an individual's adult life and its levels are defined hereditarily. Lp(a) values above 30 mg/dl increase cardiovascular risk. At present there are no specific drugs that reduce Lp(a), however, lowering LDL cholesterol with the drugs that do exist significantly reduces cardiovascular risk.
Weight loss of 5%, quantitative and qualitative moderation in fatty acid consumption, restriction of processed sugars and carbohydrates, and physical exercise 30-40 minutes 4 times per week are non-drug measures to treat dyslipidemia. Non-drug measures, although sometimes not achieving the desired result, are the cornerstone for the success of drug treatment. Nowadays there are many available hypolipidemic drugs in our therapeutic quiver. The main representative are statins along with ezetimibe and fibrates. Also omega-3 fatty acids and herbal preparations based on red rice yeast can, in certain cases of low-risk patients with mild dyslipidemia, be good allies in its treatment. Treatment is individualised for each patient depending on the hypolipidemic goals and the specificities of each patient.